There are two primary classes of visual snow. The results of a comprehensive study of visual snow are presented. The study is based on about fifty case studies that have arisen in response to this site since its inception and a subsequent close study of the relevant literature.
In the first class, labeled pulse type visual snow, extraneous dots appear scattered about the visual field suggestive of rain drops on a windshield of a car during very light rain. The dots may be darker or lighter than the average content of the scene. They may also tend to flicker individually, or to appear to swirl around in the visual field (like lines of ants).
In the second class, labeled broadband visual snow, the noise appears as a coarse texture (similar to that seen on a TV turned to a blank channel) of low amplitude obscuring the scene in object space. The noise may appear both lighter and darker than the background.
Rarely the extraneous dots appear to vary in color.
Last Update: Feb 2013
Rhodonine™ and Activa™: See Citation Page
All three of these situations are shown below, with two interpretations of analog visual snow on the right. The first shows the noise as it appears on a TV monitor close up. The second may be a more appropriate depiction of visual snow.
| PULSE TYPE VISUAL SNOW | BROADBAND (analog) VISUAL SNOW |
BLACK noise pulses.
No perceived noise
in black window frame | WHITE noise pulses.
No perceived noise
in white window frame | White noise perceived in black areas
and black noise perceived in white areas
See Rose, 1977.
| Very fine white noise as seen in the
simulation
cited below
|
It is difficult to display the symptoms of the above diseases in simple pictures because of the continual motion of the noise elements in the actual case relative to the background scene. A variety of simulations have begun to appear on the internet and have generally been prepared by Visual Snow sufferers.
Visual snow should be differentiated from the "ectopic blue field phenomenon" that involves a significantly different phenomenon and appearance. This phenomenon is explored in detail by Michael Mauser on YouTube, dated 5 April 2013. It is due to white blood cells moving in the capillaries of the retina and appear as shown below.
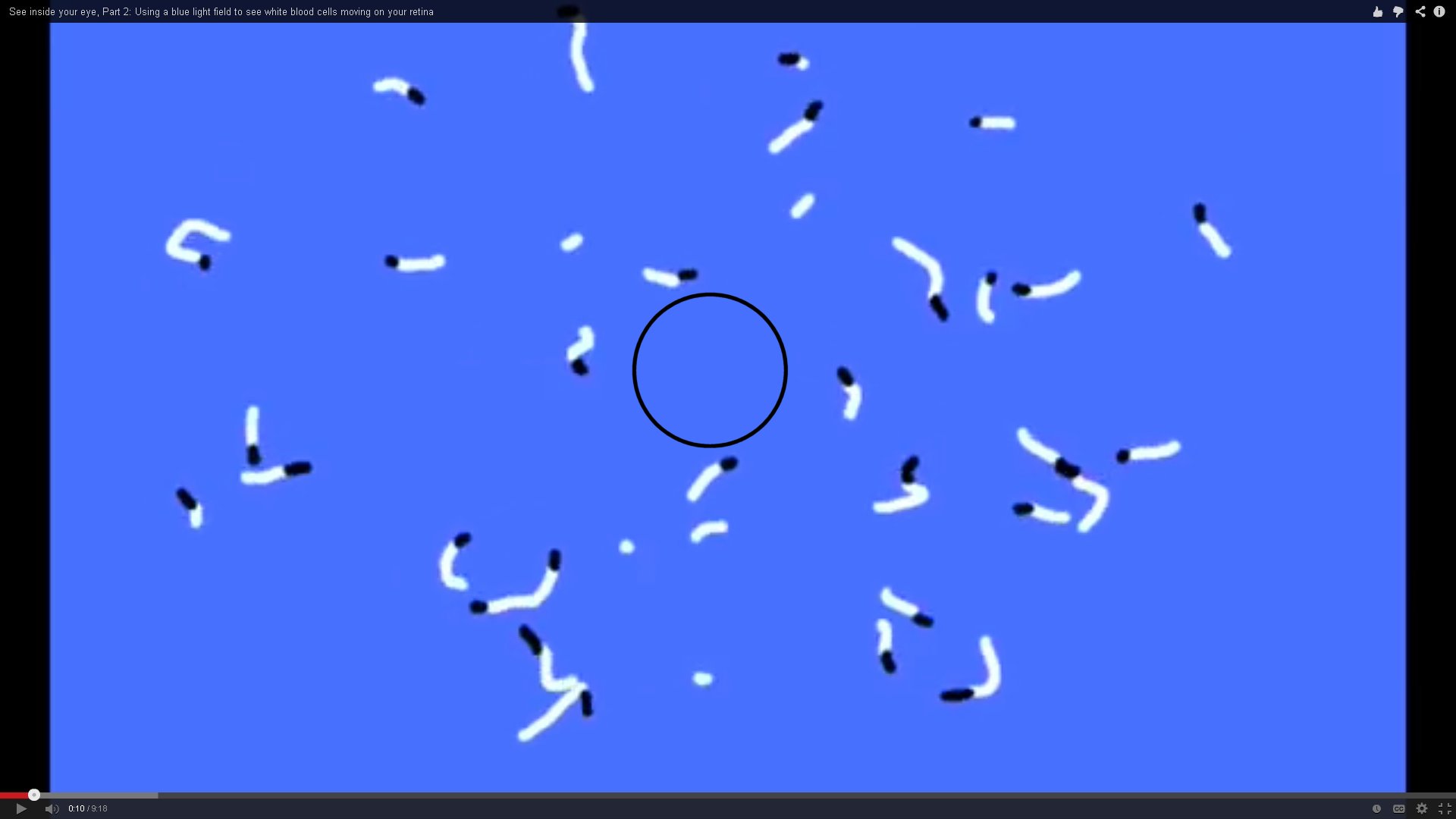 | Note the absence of any white blood cells in the very center of the field. This is diagnostic as there are no capillaries within the central foveola (1.2 degree diameter circle surrounding the point of fixation).
Most humans only see one or two of these white blood cells at a given instant and they are therefore difficult to identify. They appear and disappear in a few seconds or less.
The black dots are nominally associated with the blood cells, with the white tails representing a void in the downstrean capillary due to the large size of the white blood cells relative to other elements within the normal blood serum.
When viewing a clear blue sky, one frequently observes a mottled effect that relates to the actual noise in the vision portion of the neural system.
One may also observe low contrast ringlets, frequently connected by low contrast threads. These are typically due to dust particles on the surface of the cornea. They are necessarily viewed out of focus. |
- Physicians have had difficulty addressing Visual Snow. The condition is so rare, it is seldom seen more than once during the career of an average doctor. It is considered an orphan disease by the US National Institute of Health. After calling for an ophthalmological examination, and frequently an MRI or CT scan of the eyes, the physician will generally treat the patient for anxiety, or a more series psychosis, and ignore the actual condition. This generally causes the patient to seek opinion of another physician. The conditon does not relate to the eyes or the "primary visual cortex" and the source of the problem cannot be seen in MRI or CT images.
All VISUAL SNOW sufferers are encouraged to take the diagnostic TEST SEQUENCE in step 3 of the following list. The material in the other steps is designed for the academic or the clinician but may be read by all. The broadband and pulse type of snowy vision have distinctly separate underlying causes (etiologies) and will be discussed separately.
This page will address the following subjects;
- Major symptoms of pulse type of VISUAL SNOW
- Major symptoms of broadband type of VISUAL SNOW
- Jan 2013 Test Sequence used to quantify a subjects symptoms of VISUAL SNOW
- First Order Analyses of the Cause of the Disease
- Detailed Description of the failures leading to visual snow
- Most likely source of the extraneous signal pulses causing visual snow
- Recent scientific understanding of VISUAL SNOW
Liu, et. al. have presented an early paper (1995) describing a wide variety of persistent positive visual phenomena (labeled Aura), lasting more than seven days, that they relate to migraine headaches. They did not offer any treatment for their phenomena and noted a long list of medical tests found less than helpful in their diagnoses. This webpage will only address a specific group of their reported aura (i.e., visual snow). The symptoms discussed here last for more than seven days and are considered persistent.
As of Feb 2013, my case file contains reports from about 75 individual sufferers of Visual Snow.
Major symptoms of PULSE TYPE of visual snow
A rare disease has been reported that causes the visual field to be obscured by high frequency noise (very fine dots appearing widely spaced and at random positions over the field of view) under all conditions of illumination (including with the eyes closed in the dark).
Visual snow of the pulse type is best interpreted as a high quality image examined by looking at it through the widnow frame in one of the images on the left above.
Most of the subjects have reported the noise appears to be a veil in a plane in front of, but near, the actual image. Sometimes this plane is discontinuous, giving a stereographic effect. Only a very few subjects have defined any color aspect to the snow.
The symptoms of pulse type visual snow appear to include:
- The noise is seen as very fine asynchronous dots scattered randomly across the field of view. They do not clump in order to form larger dots.
- The dots take on the color of their background.
- The dots are not intrinsically black and white nor do they exhibit a color shift relative to the background.
- O. S. reports the contrast associated with the noise spikes is less than that displayed in the simulations of Hale. He used the term 80% transmissibility to describe the mask associated with the noise. Alternately, the dots appear to have a peak amplitude of about 20% of the scene contrast.
- The signal associated with the noise is monopolar. It can occur in either of two polarities. In the case of the "BLACK" pulse noise, the dots are always darker than the scene they obscure as illustrated on the left above. In the case of the "WHITE" pulse noise, the dots are always lighter than the scene they obscure as illustrated in the middle frame above. The "WHITE" pulse noise is most prominent under low light conditions (mesotopic and scotopic conditions).
Major symptoms of BROADBAND visual snow
Hale has summarized the broadband form of the disease within her larger syndrome quite carefully. The symptoms of the disease include the following:
- The perpetual presence of excess noise in the perceived imagery of the visual system largely independent of the illumination level but directly linked to the contrast of the scene.
- The noise appears to be spread evenly across the visual field with one possible (and if verified, important exception). Hale has reported in one instance that the noise is absent from the area of her field of view represented by her foveola.
- The signal associated with the dots is bipolar. Dark spots are observed in light areas and light spots are observed in dark areas of the scene.
- The dots are variable in size as illustrated on the right above.
As will be developed below, the broadband type of noise she describes under the title "scotopic sensitivity syndrome" appears to be closely linked to the same mechanism, but possibly not the same source as the noise in scotopic vision.
First Order Analyses of the Cause of both types of visual snow
Alison Hale has provided a web site devoted to her medical condition. Her condition is much more complicated than just exhibiting Visual Snow. Her site includes a series of four images simulating the disease of Visual Snow of the broadband type as she observes it personally. The simulations are of limited value for the purposes of this webpage. The last three images illustrate the character of the noise more clearly than the first.
Hale suggests the mechanism causing her visual snow may also cause several associated spatial perception problems that form the Hale Syndrome. She notes the basically two-dimensional perception of the world within her field of view. However, at one point, She notes that the perception of parallel lines in object space at times can become quite distorted (sometimes violently) and take on a three-dimensional character. Hale's observations have been compared with two other unrelated sufferer, O. S. and S. S. The symptoms are also comparable to those reported for subjects 6, 7, 8 & 9 in the paper by Liu, et. al. In the process of correlation, additional details about the disease have become evident, along with its potential appearance within other syndromes (groups of symptoms).
First Order Description of the Visual System
The Overall Block Diagram of the visual process in Humans and other Chordates shown below can be used to localize the failures resulting in these diseases. In the following figure, the left and right lateral geniculate nuclei (LGN) and perigeniculate nuclei (PGN) are shown along with the superior colliculus. These are all major elements of the thalamus, a portion of what is commonly called the midbrain or upper brain stem as opposed to the cerebral hemispheres. These elements receive information over the optic nerve from the eyes shown on the left and mounted on the ocular platform. Each LGN is divided into two major element called the magnocellular and parvocellular regions. The magnocellular region deals primarily with luminance information while the parvocellular region deals primarily with chrominance information. The magnocellular region also contributes significantly to the operation of the stereoptical subsystem of vision by sending signals to the superior colliculus and the ocular nuclei & oculomotor plant. These elements, along with the muscles of the eyes form the oculomotor servomechanism.
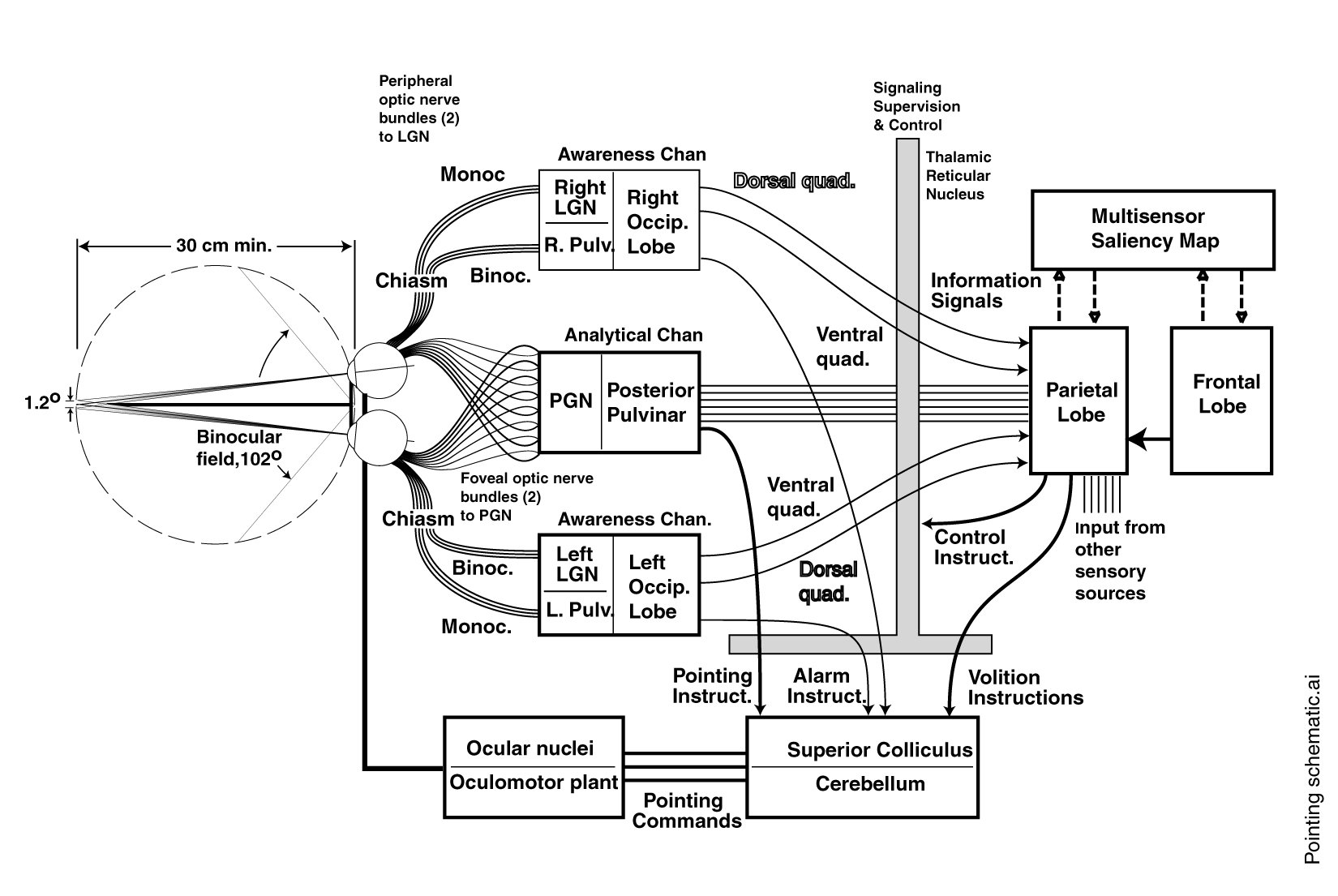
POTENTIAL FAILURE LOCATIONS IN THE OVERALL BLOCK DIAGRAM OF VISION
From figure 18.8.2-9 of Chapter 18, Section 18.8.2.
First Order Description of the Perceived Images in visual snow
A detaled description of the syndrome perceived by a subject can aid greatly in localizing the source of the abnormality in their case. A critical observation is whether one or both eyes are involved in the perception and whteher the perception is present with both eyes closed. Another critical observation concerns the even or uneven distribution of the noise across the visual field. Finally, it is very important to distinguiish between the pulse type and broadband type of visual snow. A majority of reports have described pulse type snow involving "black" noise pulses forming a veil between the subject and the external scene.
- Hale has suggested a "hole" in the noise pattern centered on her line of fixation. If this feature is confirmed, it would be significant. This hole relates to the foveola of the retina. The photoreceptors of the foveola are processed separately (by the Posterior Pulvinar in the figure) from the remainder of the retina.
- Subject S. S. has also described a nonuniformity in the noise distribution. However, he did not indicate it was centered on the line of fixation.
- In addition, S. S. has described a stereoscopic effect related to the noise pattern. He states the noise appears to be associated with a semi-transparent screen that oscillates in distance at a rate of 3-5 Hz.
- N. B. has reported from first hand experience, her visual snow only occurs in one eye (visual field of view).
An overwhelming number of participants in my survey failed to report any "hole" in their perceived visual snow corresponding to the foveola, or any distinction when only one eye was used to image a scene. The report of a stereoscopic effect is also unusual.
First Order Analyses of the Cause of both types of visual snow
Major advances have occurred in understanding the visual modality of the neural system during the first decade of the 21st Century.
My survey has been more interested in the specific representations of their perceptions because these perceptions lead to the conclusion that the source of the disease is probably in either the thalamus (particularly the thalamic reticular nucleus, TRN), the afferent signal area of the parietal lobe or in the prefrontal lobe of the cerebral cortex. There are a number of reasons to believe it does not originate in the occipital lobe of the cortex. There are also a number of reasons to believe the source of the problem is a small area of the brain that will require a very high resolution MRI facility to locate it. This suggests an MRI at higher than 3.0T will be required. A 7T or 9T MRI capable of fitting over the head only will probably be required.
The medical history of trauma and strokes affecting the occipital lobe clearly show that each section of the occipital lobe serves a separate region of the visual field. The regions are delineated into quadrants by the longitudinal cerebral fissure and the calcarine fissure. The area outside the larger circle constitutes the peripheral retina. The figure also shows that the high resolution foveola (smaller circle) is served by the pulvinar rather than the occipital lobe (frequently resulting in what is called macular sparing in the presence of severe occipital lobe damage.
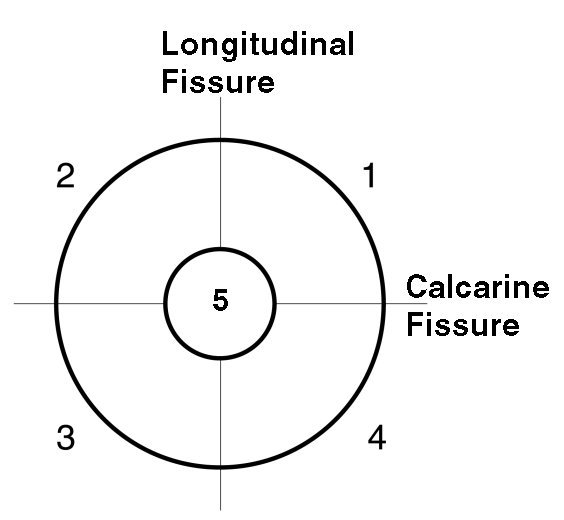
SPECIFIC PROCESSING AREAS within the human visual modality
Outer circle represents the 5.6 degree fovea.
Area 5 (1.2 degree foveola)
is an overlay of information from the
Pulvinar on the information
from the four quadrants of the
occipital lobe of the cerebral cortex.
See Section 15.6.6.2 of Chapter 15 for details
My questioning of patients centered on the above situation; "what areas of the visual field appeared snowy to them?" With one exception (Hale), the response has been the snow is distributed uniformly and without change in density across their entire visual field. These results strongly suggest the extraneous signal causing visual snow is introduced after the representations developed in these five separate areas, are combined into a single representation either within the TRN, the parietal lobe or the prefrontal lobe.
These areas are identified using a figure modified from Terese Winslow. The signals from the four distinct quadrants and the foveola are first combined in the thalamus and its outer covering (a shell), misleadingly named the thalamic reticular nucleus (TRN) located at the center of the brain just forward of, and between the left and right LGN. Once these signals are combined, they are projected to Brodmann's area 4, a portion of the parietal lobe (the probable site of the saliency map used to represent the external environment. The saliency map is accessed by the cognition engines of the prefrontal cortex (and particularly its areas that are found underneath the cerebral cortex and on its medial surfaces (not visible in the following image.
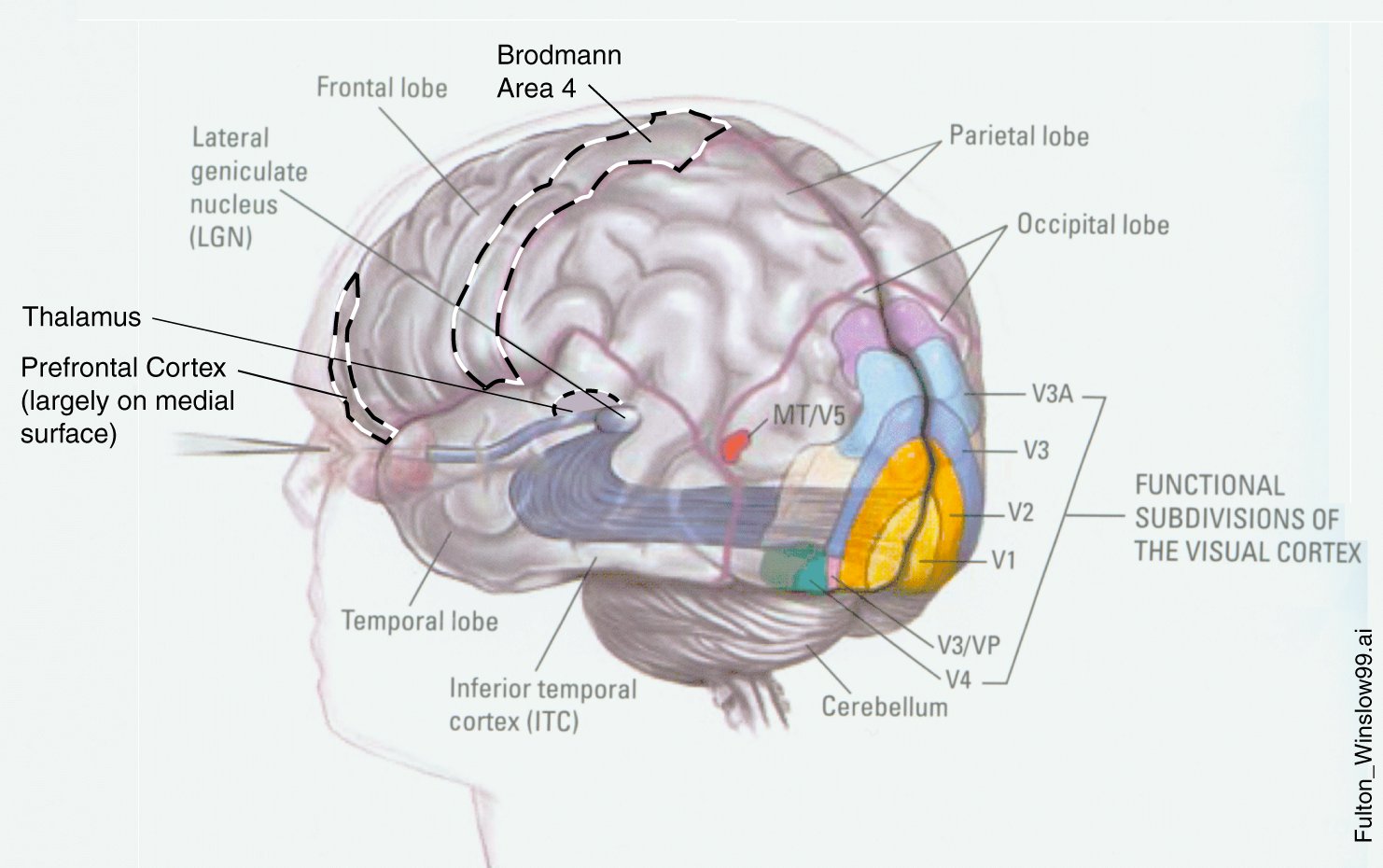
Important areas related to the origins of visual snow
If a subject checked "both" to questions 1, 2 & 3 in the Visual Snow survey on this page, it is highly likely that his disease is located within one of the areas enclosed by the dashed lines. If the subject checked lower in response to the density of the snow in his foveola (question 8a), it is highly likely his disease is located within the thalamus or TRN. His disease is likely to be found within the occipital lobe, areas labeled V1 through V4, only if he checked something other than both in response to question 2 or 3.
The symptoms of these people suffering visual snow provide pretty interesting evidence that visual snow, along with other psychedelic affects are due to changes in the local chemistry of the brain, probably due to changes in the levels of glutamic acid, GABA and dopamine-like pharmaceuticals. These changes may be ideopathic or due to either prescription or recreational drugs.
Local (sub-millimeter) changes in the chemical composition of the brain probably cannot be seen using conventional BOLD-MRI. However, they might be observable using some of the more recent differential BOLD-MRI techniques. It is probably still a long shot even at 7 Tesla MRI machines.
For more detailed information related to Visual Snow at the research level, see a draft of my Chapter 18 of "Processes in Biological Vision." Chapter 18 remains a working draft where I periodically add additional new information. http://neuronresearch.net/vision/pdf/18abnormalities.pdf
Secion 18.1.3 provides an introduction to the visual modality of the overall visual system.
- Figure 18.1.3-1 shows the effect of severing various nerves between the eyes and the cortex.
Section 18.8.2 is focused on the perception of visual snow and related perceptual distortions.
- Figure 18.8.2-1 shows an Aura establishing the separation of the foveola and the peripheral retina.
- Figure 18.8.2-2 shows an artists representation of an Aura straddling the horizontal axis (calcarine fissure) which I propose (based on personal experience and the data) is a poor representation. It should be limited to only one quadrant.
- Figure 18.8.2-5 shows how the retinal image is transferred to the occipital lobe with the horizontal axis congruent with the calcarine fissure.
- Figure 18.8.2-9 shows a high level schematic with multiple signal paths to the forward lobes of the cortex (the sections of the occipital lobe are shown separately paired with the two lateral geniculate nuclei they support.
Detailed Description of the failures leading to visual snow
Since the disease is known to arise in midlife, the cause of the problem is not likely to be genetic or of prenatal origin. Alternately, the appearance of the disease during early development suggests it is not an electrical failure (such as the creation of a unique electrical leakage path) brought on by aging. At the moment, one or more electrical bias errors, due to either chemical or hydraulic imbalance appear to be the most likely cause of these symptoms. Further perceptual tests can further isolate the location of these potential errors.
The causes described here are too subtle, and involve too small an area, to be detected using modern clinical procedures based on nuclear imaging techniques (CAT, MRI, fMRI etc.). Liu, et. al. did speculate in their Discussion that the symptoms may be due to spontaneous neural discharges.
A more complete discussion of these diseases appears below and in Chapter 18, Section 18.8.2 of PROCESSES IN BIOLOGICAL VISION. Download Chapter 18 from Table of Contents.
Details related to the PULSE TYPE of visual snow
- NOTE: The following discussion does not refer to scotopic noise that originates primarily in the stellate cells of the midbrain and is perceived under very low incident illumination of a scene in object space. Nor does it refer to photon noise which originates in the conversion of photon energy into electrical charges within the chromophores and adaptation amplifiers of the photoreceptors under mesotopic illumnation conditions. The disease is observed under all illumination conditions and is not related to the sensitivity of the eyes under scotopic conditions.
- The observation that the color of the noise does not differ significantly from the background largely eliminates the parvocellular portion of the LGN and the channels marked [P] and [Q] as a source of the failure.
- The observation that the noise pattern takes on the color of the background suggests the failure is localized to the magnocellular portion of the LGN, the channel marked [R] in the figure and the circuits of the luminance processing matrix.
- The absence of snow of a different color than the background in the perceived image of object space eliminates the photoreceptors of the retina (shown in the upper left as four parallel bars labeled L, M, S & UV) as a source of the disease.
As a result of the above observations, the source of the failure leading to PULSE TYPE visual snow can be isolated to the shaded portion of the preceding figure (including the magnocellular portion of the LGN but excluding the vertical shading leading to the three elements labeled DTN, LTN and MTN and the superior colliculus. The latter path provides the signal path that can lead to the disease of visual snow contributing to other conditions found in both Hale's Syndrome and Irlen's Syndrome.
While little known to the lay public and much of academia, the human visual system operates as a change detector and relies upon the fine motion of the eyes, known as tremor, to generate the signals used in vision. As a result of tremor, all of the pulse signals, known as action potentials, traveling over the optic nerve between the eyes and the brain are normally synchronous with the motion of the eyes. visual snow is causes by the introduction of non-synchronous action potentials into the signals carried by the individual neurons of the optic nerve. The non-synchronous nature of these action potentials makes them appear at random locations within the field of view.
Locating the source of these non-synchronous action potentials is the goal of this discussion.
Most likely source of the extraneous signal pulses causing PULSE TYPE OF visual snow
There appear to be three candidate errors leading to pulse type visual snow. First, extraneous noise can be introduced by a noise source related to the parasol ganglion cell. These potential sources are shown as ine and inp in the figure. ine stands for a noise current source in the emitter Or dendritic) lead of the Activa (the biological transistor) shown and labeled AG (Activa of the Ganglion type). inp stands for a noise current source in the poditic (or base) lead of the Activa. Second, a bias error associated with the emitter to base potential of the Activa could cause the generation of extraneous action potentials. These could be caused by an imbalance in the electrostenolytic mechanisms associated with the two rectangular boxes shown leading to the ground connections in this circuit. Third, bipolar cells are known to oscillate uncontrollably when excessive capacitance is introduced into their circuits by an investigators test probe. Such capacitance could be introduced by natural means and would lead to the observed extraneous noise.
Details related to the BROADBAND TYPE of visual snow
- NOTE: The following discussion suggests broadband type visual snow is closely related to the mechanisms associated with scotopic vision. HOwever, the source of the mechanism may be different. Normally, these mechanisms are associated with the stellate cells of the midbrain and particularly the lateral geniculate and perigeniculate nucleus (LGN & PGN). This symptom is observed under all illumination conditions and not just the low light levels normally described as scotopic.
Every time a neural signal is transmitted more than one or two millimeters, the analog information is encoded using action potentials. While encoded, the signal is largely immune to broadband noise. The recovery of this encoded signal is accomplished by the stellate cells who are always susceptable to broadband noise. However, subsequent electrotonic circuits are also susceptible to broadband noise. The fact the noise is visuotopic does suggest it occurs early in the circuitry of the LGN or PGN and is therefore likely to be due to excess noise in the stellate circuits.
A Stereoscopic hallucination closely linked to visual snow
Both A. H. and S. S. have reported stereoscopic anomalies accompanying their visual snow. The effect is analyzed in greater detail in Section 18.8.2 of CHAPTER 18 of the manuscript PROCESSES IN BIOLOGICAL VISION.
Test tablet used during Jan 2013 to quantify a subjects symptoms
The following test sequence was used to collect data from the visual snow community during January 2013. The data gathering period has ended.
The following tests are dependent on what type of visual snow you exhibit. If you exhibit black dots on a white background or broadband noise answer questions 5 and 6 using the figure below these two questions. If you exhibit white dots on a black background, answer questions 7 and 8 using the figure below these two questions.
I will soon summarize the results of this survey and make them available on this site.
I will tailor the test chart further based on the comments I receive.
Return to Table of Contents for this page.
Recent scientific understanding of VISUAL SNOW
At this time, the most likely cause of the disease known as visual snow is a chemical or hydraulic imbalance associated with the higher visual centers of the thalamus (upper brainstem), parietal lobe of the brain or the prefrontal lobe of the brain. The specific nature of this imbalance is yet to be determined. Until then, no treatment or cure for the disease can be offered. The problem is probably centered on less than 100 neurons, which is far below the resolution of current imaging techniques such as magnetic resonance imaging (MRI) or computer aided tomography (CAT).
The following remarks are prepared by a neuroscientist (researcher)and not a medical doctor (neurologist). The comments reflect the symptoms of the type of Aura known as Visual Snow collected during the author's surveys and the limited discussion of the disease in both the academic and medical literature.
Visual Snow is a hallucinogenic condition within the neural system, i.e., the subject perceives something that is not present in the actual visual scene presented to the sensory system.
Visual snow is typically reported to be present continuously, even with both eyes closed (and even while dreaming according to some reports). The perception of visual snow is sometimes reduced depending on the level of attention of the individual to specific taskes.
The appearance of visual snow in color, particularly like confettiin the case of broadband visual snow is unusual. Because of the small size of the dots in impulse type visual snow, colored snow of this type is seldom reported and probably anecdotal.
Every indication suggests Visual Snow arises in the higher level areas of the central nervous system (the brain) and not in the eyes or the lower levels of information extraction, such as the occipital lobe of the CNS (also known as the primary visual cortex).
Analysis of all of the relevant information assembled above indicates the source of Visual Snow appears to be a small group of neurons within either;
- The higher stage 4 levels of information extraction associated with the thalamic reticular nucleus (TRN) surrounding the thalamus within the midbrain (diencephelon).
- The high level stage 4 representation of the visual information assembled in the saliency map believed to be present in the stage 4 circuits of the afferent portion of the parietal lobe.
- The high level stage 5 cognition circuits of the prefrontal lobe of the CNS responsible for interpreting the information supplied to it by the saliency map.
- The stage 3 signal projection (action potential circuits) circuits interconnecting the stage 4 and stage 5 analog information processing engines.
A failure within the stage 3 signal projection circuits is believed to result in the pulse type of visual snow.
A failure within the analog circuits of the stage 4 (information extraction) or stage 5 (cognition) engines of the CNS is believed to result in the broadband type of visual snow.
The major cause of Visual Snow appears to be an abnormal flow of chemical nutrients, particuarly glutamic acid to and gamma amino butyric acid (GABA) away from, a very small group of neurons (probably less tha 100 in each case) within the central nervous system (CNS). These chemicals are instrumental in providing the electrical biasing of the electrolytic neurons. The result is abnormal operation of these neurons.
While such abnormal flows can be genetic in nature, this is not the predominant case. The condition typically arises due to ingestion of a variety of pharmaceutical preparations, whether medically prescribed or taken in the form of recreational drugs. It may also arise through trauma to the brain or infarcation (a stroke). In some cases, it may be a result of the aging process. However, it typically arises rather abruptly.
The -mycin class of antibiotics (kanamycin and neomycin among others) are implicated but not statistically demonstrated to be the cause of visual snow when used in excessive amounts because of their known impact on the related Aura of tinnitus.
A variety of opioids (both prescribed and used as recreational drugs) are implicated but not statistically demonstrated to be the cause of visual snow when used in excess because of their frequent use in the adolescent population prior to the appearance of a variety of Aura including visual snow.
The perception of visual snow does not appear to worsen significantly following its initial appearance. It is generally not progressive. On the other hand, visual snow rarely disappears once it appears.
Until a very highly targeted medical treatment for the condition is developed, it is not likely to be curable. The reason is that most treatments to correct the abnormal local chemical flow within the CNS are likely to cause abnormal conditions (side effects) elsewhere within the CNS.
Return to Table of Contents for this page.
Return to the CLINICAL Home Page .
Return to the NEURON Home Page .
Return to the VISION home page
References
Liu, G. et. al. (1995) Persistent positive visual phenomena in migraine, Neurology, vol. 45, pages 664-668
Liu, G. Volpe, N. & Galetta, S. (2001) Neuro-Ophthalmology. NY: Saunders
Rose. A. (1977) Vision: Human versus Electronic in Barlow, H. & Fatt, P. Vertebrate Photoreception NY: Academic Press pp 1-13
Sacks, O. (1992) Migraine Berkeley, CA: University of California Press